
If you or a loved one has been told you have “high myopia,” you might feel a mix of confusion and concern. Is it just severe nearsightedness? Does it mean you’re going blind? First, take a deep breath. While high myopia is a serious eye condition that requires attention, it is highly manageable with today’s medical advancements.
In 2025, we know more about myopia than ever before. It isn’t just about needing a stronger prescription; it’s about the physical shape of your eye and how to protect your long-term vision. This comprehensive guide breaks down everything you need to know—from the latest treatment options to practical lifestyle tips—in plain English, backed by the latest medical standards.
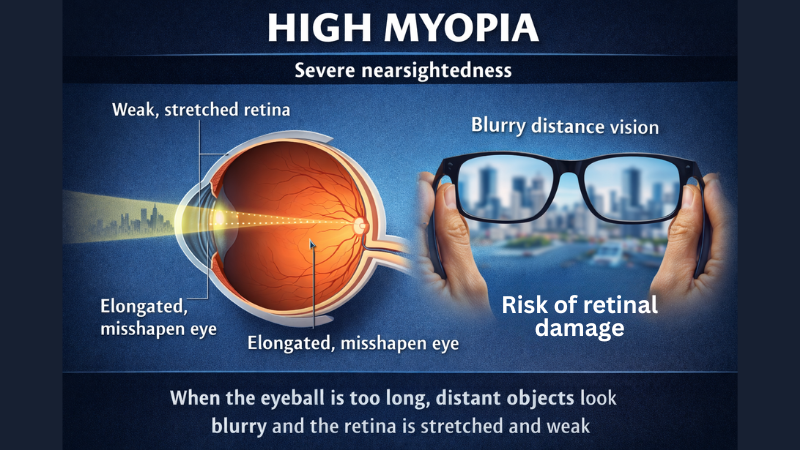
What Is High Myopia? (The Medical Definition)
Myopia (nearsightedness) occurs when the eye grows too long, causing light to focus in front of the retina rather than directly on it. This makes distant objects look blurry.
High myopia is the severe form of this condition. In medical terms, it is generally defined by two key metrics:
- Refractive Error: A prescription of -6.00 diopters (D) or higher.
- Axial Length: An eyeball length of 26.5 mm or longer.
Note for Parents: High myopia usually develops in childhood and worsens progressively. However, updated 2025 guidelines emphasize that “myopia control” strategies can significantly slow this progression if started early.
High Myopia vs. “Pathological” Myopia
It is crucial to distinguish between the two:
- High Myopia: You have a high prescription (-6.00D+), but your retina and eye structures may still look relatively healthy.
- Pathological Myopia: The excessive stretching of the eye causes structural damage (degenerative changes) to the retina, choroid, and optic nerve. This affects only a subset of high myopes but is a leading cause of visual impairment.
Causes and Risk Factors: Why Me?
Why do some people need mild reading glasses while others have high myopia? It’s usually a “perfect storm” of genetics and environment.
- Genetics: If both parents are nearsighted, a child’s risk increases significantly. However, genetics alone doesn’t explain the global surge in cases.
- Visual Environment: This is the biggest driver in the modern world.
- Near Work: Extensive reading, studying, and screen time force the eye to focus up close for hours, signaling it to elongate.
- Lack of Outdoors: Research consistently shows that a lack of exposure to natural sunlight (specifically the intensity of outdoor lux) disrupts the dopamine regulation that stops the eye from growing too long.
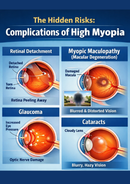
The Hidden Risks: Complications of High Myopia
This section is critical. High myopia is not just an inconvenience; it is a medical condition that changes the anatomy of your eye. The stretching of the eyeball thins the retina (the light-sensitive layer at the back of the eye), making it more vulnerable.
1. Retinal Detachment
Because the retina is stretched thin, it is more prone to tearing. Fluid can seep through a tear and lift the retina off the back of the eye.
- The Stat: High myopes have a significantly higher risk of detachment compared to the general population.
- Warning Signs: Sudden flashes of light, a shower of new floaters, or a “curtain” falling over your vision. This is a medical emergency.
2. Myopic Maculopathy (Macular Degeneration)
This affects the macula, the center of the retina responsible for sharp, detailed vision. The stretching can cause atrophy (wasting away) or new, leaky blood vessels to form.
3. Glaucoma
High myopia changes the structure of the optic nerve, making it more susceptible to pressure damage. Glaucoma is often called the “silent thief of sight” because it has no early symptoms.
4. Cataracts
While cataracts are a normal part of aging, they tend to develop 10–15 years earlier in people with high myopia.
Diagnosis: What to Expect in 2025
A standard vision test at the mall isn’t enough. If you have high myopia, you need a comprehensive dilated eye exam at least once a year.
The “Gold Standard” Exam Includes:
- Dilated Retinal Exam: The doctor uses drops to widen your pupil and examine the periphery of your retina for thinning (lattice degeneration) or tiny holes.
- Axial Length Measurement: Just as we measure a child’s height, measuring the length of the eye (optical biometry) is now standard for tracking progression.
- OCT (Optical Coherence Tomography): An ultrasound-like scan that creates cross-sectional images of your retina to check for early signs of macular damage.
Treatment and Management Options
Managing high myopia falls into two categories: vision correction (seeing clearly now) and myopia control (stopping it from getting worse).
1. Vision Correction (Adults)
- High-Index Lenses: Gone are the days of “coke-bottle” glasses. High-index materials allow for thinner, lighter lenses even for strong prescriptions.
- Contact Lenses: RGP (Rigid Gas Permeable) and Scleral lenses often provide sharper vision than soft contacts for high myopes because they mask corneal irregularities.
- Refractive Surgery (LASIK / PRK / SMILE):
- Caution: There is a limit to how much tissue can be removed. If your corneas are too thin or your prescription is too high (usually over -8.00D or -9.00D), laser surgery might not be safe.
- ICL (Implantable Collamer Lens): For extreme myopia (up to -20.00D), surgeons can implant a permanent lens inside the eye. This preserves the cornea and offers excellent visual quality.
2. Myopia Control (Children & Teens)
If you have a child whose prescription is changing rapidly, standard glasses are no longer the standard of care. 2025 protocols favor active management:
- Orthokeratology (Ortho-K): Wearing hard contact lenses overnight to reshape the eye. It corrects vision for the day and signals the eye to stop growing.
- Low-Dose Atropine Drops: A nightly eye drop (0.01% to 0.05%) that relaxes the focusing mechanism and hardens the sclera to prevent elongation.
- Myopia Control Glasses/Contacts: New specialized lenses (like defocus incorporated multiple segments) blur peripheral vision slightly to trick the eye into stopping growth.
- Red Light Therapy: An emerging therapy involving looking into a specialized red light device for a few minutes daily, showing promising results in thickening the choroid and slowing growth.
Living with High Myopia: Lifestyle Tips
You cannot shrink your eye back to normal size, but you can protect the vision you have.
- The 20-20-20 Rule: For every 20 minutes of near work, look at something 20 feet away for 20 seconds. This relaxes the ciliary muscle.
- Get Outdoors: Aim for 2 hours of outdoor time daily. The brightness of natural light (even on cloudy days) is beneficial.
- Avoid Eye Rubbing: Vigorously rubbing your eyes can spike eye pressure and mechanically stress a thin retina.
- Blue Light & Screens: While blue light itself isn’t the primary enemy, the proximity of screens is. Keep phones and tablets at least an arm’s length away.
Conclusion: A Proactive Approach
High myopia is a lifelong journey, but it doesn’t have to define your life. The narrative has shifted from “bad eyes” to “structural eye health.”
Your Next Steps:
- Check your prescription: If you are over -6.00D, ensure you are seeing a retina specialist or an optometrist who specializes in myopia management.
- Schedule an exam: If it’s been more than 12 months since your last dilated exam, book one today.
- Kids: If you are a parent with high myopia, get your children checked early (by age 3-5) and ask about myopia control immediately if they show signs of nearsightedness.
Frequently Asked Questions (FAQs)
Can high myopia be cured?
No, high myopia cannot be “cured” because the physical elongation of the eyeball is permanent. However, it can be corrected with lenses or surgery, and its progression can be slowed in children.
Is high myopia a disability?
High myopia itself is not usually classified as a disability if it can be corrected to 20/20 with glasses or contacts. However, if complications like myopic maculopathy cause uncorrectable vision loss, it may be considered a visual impairment.
Can I play sports with high myopia?
Yes, but protection is key. Because you are at higher risk for retinal detachment, you should wear sports goggles (polycarbonate lenses) for contact sports. Avoid high-impact activities like boxing or bungee jumping where head trauma is likely.
Will I definitely get a retinal detachment?
No. While the risk is higher (statistics vary, but roughly 1 in 20 to 1 in 50 depending on severity), the majority of people with high myopia do not suffer a detachment. Regular exams allow doctors to spot and laser-seal weak areas before they detach.











