What This Guide Covers
Choosing how to correct your vision shouldn’t feel like a maze. This guide walks you through every major option—glasses, contact lenses, orthokeratology, laser eye surgery (PRK, LASIK, SMILE), implantable lenses (ICL), and lens-based procedures (RLE, cataract IOLs). We’ll compare who each option is for, what to expect, safety considerations, and long-term value for vision correction options.
Who This Is For
If you’re weighing costs, comfort, lifestyle, and clarity—and want an easy-to-understand, no-jargon overview—you’re in the right place. Whether you’re a student who hates fogging glasses, a professional glued to screens, or someone finally ready to ditch readers, there’s a tailored path for you.
Understanding Refractive Errors
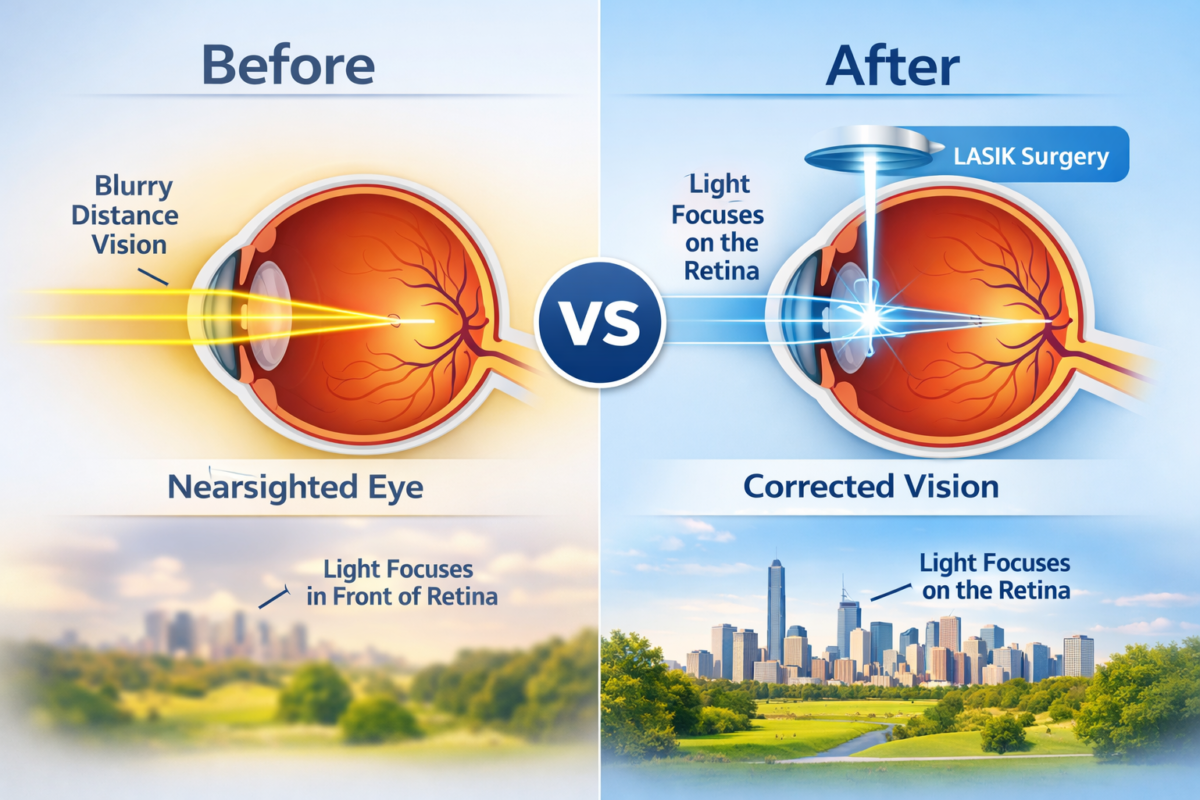
Your eye focuses light onto the retina. When the shape of the cornea or lens doesn’t bend light just right, images blur. Each “error” has its own pattern and solution.
Myopia (Nearsightedness)
Distant objects blur; near tasks are clearer. Common in screen-heavy lifestyles and often progresses during childhood and teens.
Hyperopia (Farsightedness)
Near tasks strain; distance can be okay but not perfect. Headaches after reading? This might be why.
Astigmatism
The cornea isn’t perfectly round, so vision can blur at all distances. It’s correctable in glasses, contacts, and most refractive surgeries.
Presbyopia
Starting around the 40s, the eye’s natural lens loses flexibility. Reading gets tougher, and you might find yourself stretching your arms for focus.
How to Choose the Right Option
Think of this as a quick decision framework.
Lifestyle Factors
- Hate maintenance? Glasses or LASIK may suit you.
- Play contact sports? Consider contacts, ortho-K, or laser options.
- Night driving a lot? Discuss glare/halo risk and lens choices with your doctor.
Eye Health & Suitability
- Dry eye? That can affect contact lens comfort and surgical outcomes.
- Thin corneas? LASIK may be limited; PRK, SMILE, or ICL could be better.
- Irregular corneas or keratoconus? Scleral lenses or CXL-based approaches may be key.
Budget & Long-Term Costs
Glasses seem cheap, but premium lenses add up over years. Contacts have recurring costs. Surgery has higher upfront cost but can pay off over time—especially if you currently buy specialty lenses or multiple pairs.
Realistic Expectations
No option is perfect. The goal is the best mix of clarity, convenience, safety, and cost for you.
Eyeglasses
Still the simplest, safest way to sharpen vision—and a fashion accessory if you want.
Lens Types: Single-Vision, Bifocal, Progressive
- Single-Vision: One prescription for all distances (great for myopia/hyperopia).
- Bifocal: Two zones—distance and near—separated by a visible line.
- Progressive: A smooth, no-line gradient from distance to near.
Advanced Lens Materials & Coatings
- High-index materials thin heavy prescriptions.
- Anti-glare/anti-reflective coatings improve clarity and night driving.
- Photochromic lenses darken outdoors.
- Blue-light coatings can reduce reflections and eye strain for some users.
Pros, Cons, and Best For
- Pros: Zero contact with the eye; easy; safe; cost-flexible.
- Cons: Fogging, frame weight, limited side vision with certain frames.
- Best For: Anyone prioritizing safety and low maintenance.
Contact Lenses
Contacts give natural field of view and freedom from frames—if you’re disciplined about hygiene.
Soft Lenses (Daily, Bi-weekly, Monthly)
- Daily disposables: Maximum hygiene and convenience; great for allergies or infrequent wear.
- Bi-weekly/Monthly: Cost effective but demand consistent cleaning.
Toric & Multifocal Lenses
- Toric designs correct astigmatism.
- Multifocal lenses target presbyopia so you can see distance and near.
Rigid Gas Permeable (RGP) & Scleral Lenses
- RGP: Crisp optics, durable, great for high astigmatism; adaptation needed.
- Scleral: Larger lenses that vault the cornea, ideal for keratoconus or irregular corneas, and surprisingly comfy once fitted.
Pros, Cons, and Best For
- Pros: Wider field, sports-friendly, no fogging.
- Cons: Hygiene burden; dry eye challenges; replacement costs.
- Best For: Active lifestyles, cosmetic preference, and precise optics needs.
Orthokeratology (Ortho-K)
Sleep in specially designed rigid lenses that temporarily reshape the cornea. Wake up and see without daytime lenses or glasses.
How Overnight Corneal Reshaping Works
Custom lenses gently flatten central cornea overnight. Remove in the morning and get all-day clarity (typically for mild-to-moderate myopia and some astigmatism).
Who Makes a Good Candidate
- Mild–moderate myopia
- Active days (sports, dusty workplaces)
- Motivated to clean and care for lenses meticulously
Benefits, Risks, Maintenance
- Benefits: Daytime freedom; reversible if stopped; helpful for some children in slowing myopia progression.
- Risks: Infection if hygiene lapses; initial adaptation.
- Maintenance: Strict cleaning; routine follow-ups.
Laser Eye Surgery
All laser procedures reshape the cornea to refocus light. The differences are in approach, recovery, and candidacy.
PRK (Photorefractive Keratectomy)
- How it works: The surface epithelium is removed; a laser reshapes the cornea; a bandage lens helps healing.
- Pros: No flap; good for thinner corneas; stable outcomes.
- Cons: A few days of discomfort; slower visual recovery than LASIK.
- Best for: Physically demanding jobs, contact sports, thinner corneas.
LASIK (Laser-Assisted In Situ Keratomileusis)
- How it works: A thin flap is created, the underlying cornea is reshaped, and the flap is repositioned.
- Pros: Rapid recovery; minimal discomfort; highly predictable.
- Cons: Rare flap complications; dryness in the short term.
- Best for: Broad range of myopia/hyperopia/astigmatism if cornea thickness is adequate.
SMILE (Small Incision Lenticule Extraction)
- How it works: A small keyhole incision removes a lenticule (a tiny disk of tissue) to reshape the cornea—no flap.
- Pros: Small incision; often less dryness; quick return to activities.
- Cons: Currently most established for myopia/astigmatism (hyperopia indications vary by region).
- Best for: Active individuals, dry-eye-prone patients, those favoring no flap.
Which Laser Procedure Fits Which Profile
- Thin cornea or high-impact sports: PRK or SMILE
- Need fastest recovery: LASIK
- Dry eye concerns: Consider SMILE or PRK with ocular surface optimization
Corneal Cross-Linking (CXL) for Keratoconus
CXL isn’t a vision-correction procedure per se—it’s a stabilization treatment.
When CXL Is Used
For progressive keratoconus or corneal weakening, CXL strengthens corneal collagen to halt progression.
CXL + Vision Correction Options
After stabilization, many patients do well with scleral lenses for crisp vision. Some may consider topography-guided PRK in carefully selected cases once stable, as advised by a cornea specialist.
Phakic IOLs / ICL (Implantable Collamer Lens)
Think of ICL as a contact lens implanted inside the eye, in front of your natural lens.
How ICL Works
A surgeon inserts a thin, biocompatible lens through a tiny incision. It corrects myopia (and toric versions correct astigmatism) without removing corneal tissue.
Who Benefits Most
- High myopia not ideal for laser procedures
- Thin corneas or dry-eye-prone individuals
- Those wanting a reversible option (ICL can be removed/changed)
Pros, Cons, and Recovery
- Pros: Excellent optics; rapid recovery; preserves cornea.
- Cons: Intraocular surgery risks (though low in experienced hands); periodic checks for pressure and vault.
- Recovery: Usually quick—visual improvement is fast, with routine follow-ups.
Refractive Lens Exchange (RLE) & Cataract Options
RLE is like cataract surgery performed before a cataract becomes visually significant.
Monofocal, Multifocal, and Toric IOLs
- Monofocal: Clear focus at one distance, usually far; readers for near.
- Toric: Corrects corneal astigmatism at the same time.
- Multifocal/EDOF: Aim to reduce dependence on glasses at multiple distances (distance, intermediate, and near), with some trade-offs like halos for a subset of patients.
Monovision vs. Multifocal Strategies
- Monovision: One eye set for distance, the other for near; brain blends images. Try with contact lenses first to see if you like it.
- Multifocal/EDOF IOLs: Both eyes aim for broader range of focus; good lighting and neuroadaptation help.
Candidacy, Risks, and Recovery
- Candidacy: Often for presbyopes (40s+) prioritizing glasses independence, especially those with early lens changes.
- Risks: Glare/halos (usually reduce over time), dry eye flares, rare surgical complications.
- Recovery: Typically quick; vision improves over days to weeks.
Presbyopia Solutions Without Surgery
Not ready for a procedure? You’ve got options.
Reading Glasses & Progressives
Affordable, simple, and reliable. Progressives avoid swapping glasses by blending distances.
Contact Lens Monovision & Multifocal Designs
A great test-drive for presbyopia strategies before committing to surgery. Many professionals trial these before discussing RLE/IOLs.
Special Cases: High Prescriptions & Irregular Corneas
When numbers are big or corneas are uneven, a custom plan matters.
Keratoconus & Post-Surgical Irregularity
Scleral lenses often deliver the sharpest, most comfortable vision by creating a smooth optical surface. Combine with CXL for stability when progression is present.
Scleral Lenses vs. Surgery
If corneas are irregular, optics from a well-fit scleral lens can beat surgery for clarity. Surgery may still help some—but only after careful topography and specialist input.
Dry Eye & Ocular Surface Considerations
Why Tear Film Matters
Your tear film is the first optical surface. If it’s unstable, vision fluctuates—no matter the correction method.
Optimizing the Surface Before Surgery or Contacts
Treat dry eye before fittings or surgery to improve comfort, accuracy of measurements, and final results. This can include lubricants, lid hygiene, punctal plugs, meibomian gland care, or lifestyle changes.
Safety, Risks, and Realistic Outcomes
Common Side Effects by Option
- Glasses: Distortion at lens edges with strong prescriptions.
- Contacts: Dryness, infections if hygiene lapses.
- PRK/LASIK/SMILE: Temporary dryness, glare/halos; rare complications.
- ICL/RLE: Intraocular surgery risks; halos/glare more likely with multifocal IOLs initially.
Managing Night Vision & Halos
Good tear film, proper pupil-cornea matching, and realistic lighting expectations matter. Techniques and technologies continue to improve; discuss night-driving needs with your surgeon.
Enhancements and Re-treatments
Even after surgery, small residual prescriptions can occur. Enhancements are sometimes possible once vision stabilizes, depending on corneal thickness and overall ocular health.
Costs & Long-Term Value
Upfront vs. Ongoing Costs
- Glasses: Lower upfront; recurring costs for upgrades and spares.
- Contacts: Moderate ongoing expense (lenses, solutions, exams).
- Surgery (PRK/LASIK/SMILE/ICL/RLE): Higher upfront; minimal recurring costs, though dry eye care or enhancements may add expenses.
Insurance, Financing & HSA/FSA Tips
Many plans treat refractive surgery as elective, but tax-advantaged accounts can help. Some centers offer payment plans. Toric/multifocal IOLs may carry additional fees during cataract surgery.
Preparing for Your Consultation
What Tests to Expect
- Refraction & keratometry (your exact prescription and corneal curvature)
- Topography/tomography (maps of corneal shape/thickness)
- Pupil size & tear film evaluation
- Retinal exam to rule out other issues
Questions to Ask Your Eye Doctor
- Which options match my cornea thickness and tear film?
- What night-vision outcomes should I expect?
- If I get surgery now, how will presbyopia be handled later?
- What is the enhancement policy and cost?
Aftercare & Maintenance
Recovery Timelines
- Glasses: Instant.
- Contacts: A few days to adapt for RGPs; soft lenses are immediate.
- PRK: Functional vision in days; sharper over weeks.
- LASIK/SMILE: Usually clear within 24–72 hours.
- ICL/RLE: Quick improvement, fine-tuning over days to weeks.
Hygiene & Follow-ups
- Contacts/Ortho-K: Clean daily, replace as directed, never sleep in lenses unless prescribed (like ortho-K).
- Surgery: Use drops as directed, avoid rubbing eyes, attend all follow-ups.
Conclusion
There’s no one “best” vision correction option—there’s the best fit for your eyes, lifestyle, and goals. Glasses are safe and simple. Contacts provide freedom with responsibility. Ortho-K unlocks daytime clarity without daytime lenses. Laser procedures (PRK/LASIK/SMILE) offer fast, reliable independence from eyewear for many. ICL and RLE extend solutions to high prescriptions and presbyopia, while CXL helps stabilize corneas when needed. Pair the right technology with healthy ocular surface care, and you’ll see the world the way you want—clearly, comfortably, and confidently.
FAQs
Q1. Which vision correction option is the safest?
A: Safety depends on candidacy and compliance. Glasses have the lowest risk. For procedures, outcomes are excellent when you’re properly screened and follow instructions. Your surgeon’s experience and your ocular surface health are key.
Q2. Can laser eye surgery fix astigmatism?
A: Yes. Modern PRK, LASIK, and SMILE correct many levels of astigmatism. Candidacy depends on corneal thickness, shape, and overall eye health.
Q3. I’m over 40—should I wait for cataracts or consider RLE now?
A: It depends on your priorities. If you want fewer glasses now and have early lens changes, RLE can make sense. Otherwise, laser surgery plus readers later is a common path. A consultation can map out both scenarios.
Q4. Will I still need glasses after surgery?
A: Maybe for certain tasks, especially close work if you choose distance-focused correction. Multifocal/EDOF IOLs or monovision strategies can reduce dependence further, but trade-offs exist.
Q5. I have dry eyes. Which options work best?
A: Start by treating the dry eye first. Daily disposable contacts, SMILE or PRK (with surface optimization), ICL, or simply high-quality glasses may all be comfortable once the tear film is stabilized.