In 2026, childhood myopia (nearsightedness) is no longer seen as just a “need for glasses”—it is recognized as a progressive condition that requires active management to protect long-term eye health. The following article is designed for parents and patients to understand the science, treatment options,
MYOPIA:
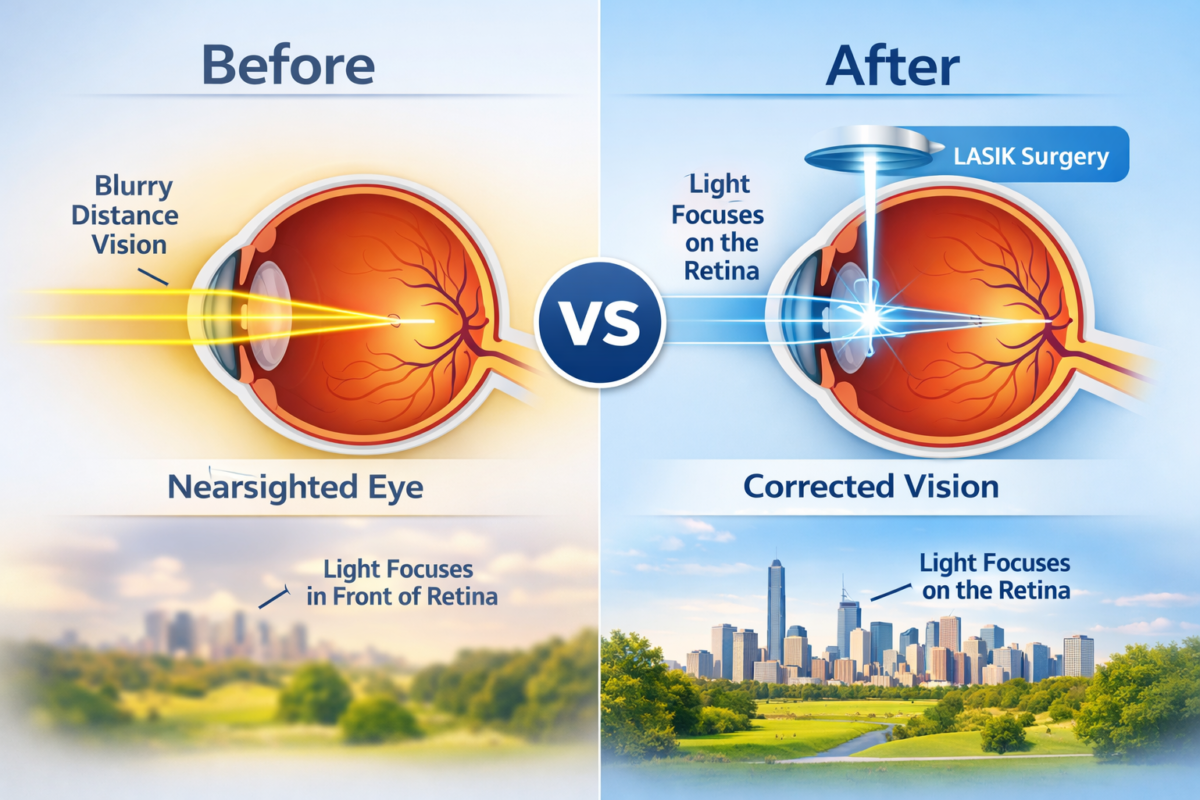
Myopia occurs when the eyeball grows too long (axial elongation) or the cornea is too curved. This causes light to focus in front of the retina instead of directly on it, making distant objects look blurry while close-up tasks remain clear.
Why Is Myopia Increasing?
The “Myopia Epidemic” is driven by two main factors:
- Genetics: A child with one myopic parent is 3x more likely to develop it; with two myopic parents, the risk jumps to 6x.
- Lifestyle: Modern “near-work” (tablets, phones, reading) and a lack of outdoor sunlight are the primary environmental triggers. Sunlight triggers dopamine release in the retina, which naturally slows down eye growth.
The 2025 Myopia Management Toolkit:
Historically, we only “corrected” vision with standard glasses. Today, we manage it using treatments proven to slow progression by 50% to 60%.
| Treatment | How it Works | Best For |
| Low-Dose Atropine | Daily eye drops that signal the eye to slow its growth. | Young children or those not ready for contacts. |
| Ortho-K (Overnight Lenses) | Hard lenses are worn only while sleeping to reshape the cornea. | Active kids and swimmers; provides clear vision all day without glasses. |
| MiSight® 1-Day | Specialized soft contact lenses are worn during the day. | Children aged 8+; the first FDA-approved lens for myopia control. |
| Defocus Glasses | New-gen spectacle lenses (like DIMS or HALT technology). | Children who prefer glasses over contact lenses. |
AI in Myopia: The New Frontier:
Artificial intelligence is transforming how we treat nearsightedness. In 2025, eye care professionals use AI for:
- Progression Prediction: AI algorithms analyze a child’s age, lifestyle, and eye measurements to create a “growth chart.” This predicts exactly how high their prescription might go by age 18 if left untreated.
- Personalized Treatment: AI helps doctors choose the specific treatment (e.g., 0.025% vs. 0.05% atropine) that is most likely to work for your child’s unique eye structure.
- Early Screening: AI-powered retinal cameras in schools can now detect “pre-myopia” before the child even realizes their vision is blurry.
Parent Checklist: Spotting the Signs:
Children often don’t complain about blurry vision because they think everyone sees the way they do. Watch for:
- Squinting while watching TV or looking at the board.
- Sitting very close to screens or holding books near the face.
- Frequent headaches or eye rubbing after school.
- Disengagement in sports or activities that require distance vision.
Frequently Asked Questions (FAQ):
Q: Can my child just “grow out” of myopia? A: No. Unlike some conditions, myopia typically only gets worse as the child grows. The goal is to “freeze” or slow the progression during the peak growth years (ages 6–15).
Q: Are contact lenses safe for an 8-year-old? A: Yes. Research shows that children are often more compliant with hygiene than teenagers. Modern daily disposables like MiSight significantly reduce the risk of infection.
Q: Is “screen time” the only culprit? A: Not exactly. It’s the intensity of near work and the lack of outdoor light. The “20-20-20 Rule” (every 20 minutes, look 20 feet away for 20 seconds) is the best defense.
Q: What is the biggest risk of “high myopia”? A: If the eye grows too long, the tissues stretch and thin. This increases the lifetime risk of retinal detachment, glaucoma, and macular degeneration in adulthood.
Actionable Tips for Parents:
- 90–120 Minutes Outdoors: Aim for 2 hours of outdoor time daily (sunlight is the key).
- The 20-20-20 Rule: Set a timer during homework or tablet use.
- Regular Eye Exams: Don’t rely on school screenings; they often miss 1 in 4 vision issues. A comprehensive exam with axial length measurement is the gold standard.